
Health care is a consistently supply-oriented industry. The business models, operating models, and even the patient experiences revolve around the supplier—that is, the provider and the services the provider or health care organization offer the patient. Vaccines are no exception. And the approach isn’t working.
So, when it comes to addressing vaccine hesitancy, especially for childhood vaccines, it’s clear we need a different approach. Supply-side messaging isn’t going to move the demand side of the equation. So what can we do instead?
The current state of childhood vaccination in the U.S.
Vaccination levels are falling (i.e., people are “firing” vaccinating their children). The problem isn’t that vaccine skepticism and the associated reduction in childhood vaccines is new. It’s not. The problem is that it’s growing. This chart from The New York Times displays the trend well:
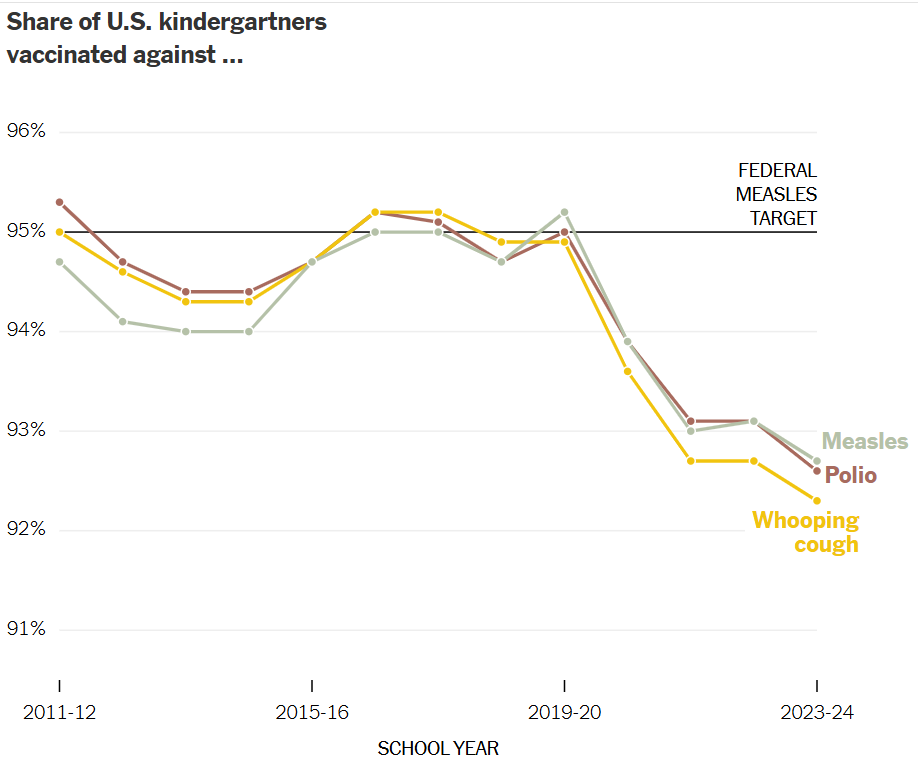
As vaccination rates are still in the 90s, the good news is that the majority of parents are still pro-vaccine. But it’s not guaranteed to stay that way, especially in today’s changing landscape.
A logical question for those of us wedded to the evidence base is: why are people hesitant to vaccinate their children? We think the science is clear. Vaccines are overwhelmingly safe, which doesn’t mean they come with zero risk (almost nothing does), and they overwhelmingly prevent diseases that used to kill children en masse.
But if public health, health care, and scientific officials want childhood vaccination rates to rise, we need to shift our message. Saying “vaccines save lives” isn’t enough. Instead, we must acknowledge people’s circumstances and their emotional, social, and functional desires for progress. In Christensen’s words, we must understand their Jobs to Be Done. And that starts with understanding people’s current circumstances.
A big part of our current situation, and part of what contributes to vaccine hesitancy, is that we’ve collectively forgotten the past. This perspective puts our risk assessment out of balance.
We’ve forgotten just how deadly the past was for children
When it comes to assessing the current risk of bad outcomes, or even death, forgetting the past allows us to worry about the smaller-than-death negative outcomes of vaccines while discounting the upside gain of children surviving childhood. We now take for granted that our children will survive childhood, but that’s only a given if we continue to hire life-saving vaccines.
The reason we likely take childhood survival for granted is that the parents choosing to vaccinate their children today—or not—have no memory of a world where children routinely came down with polio, measles, diphtheria, etc. Notably, one member of Congress old enough to live before a widespread polio vaccine is Mitch McConnell, who contracted the disease as a child, and he voted against confirming a vaccine skeptic as head of Health and Human Services (HHS). He remembers.
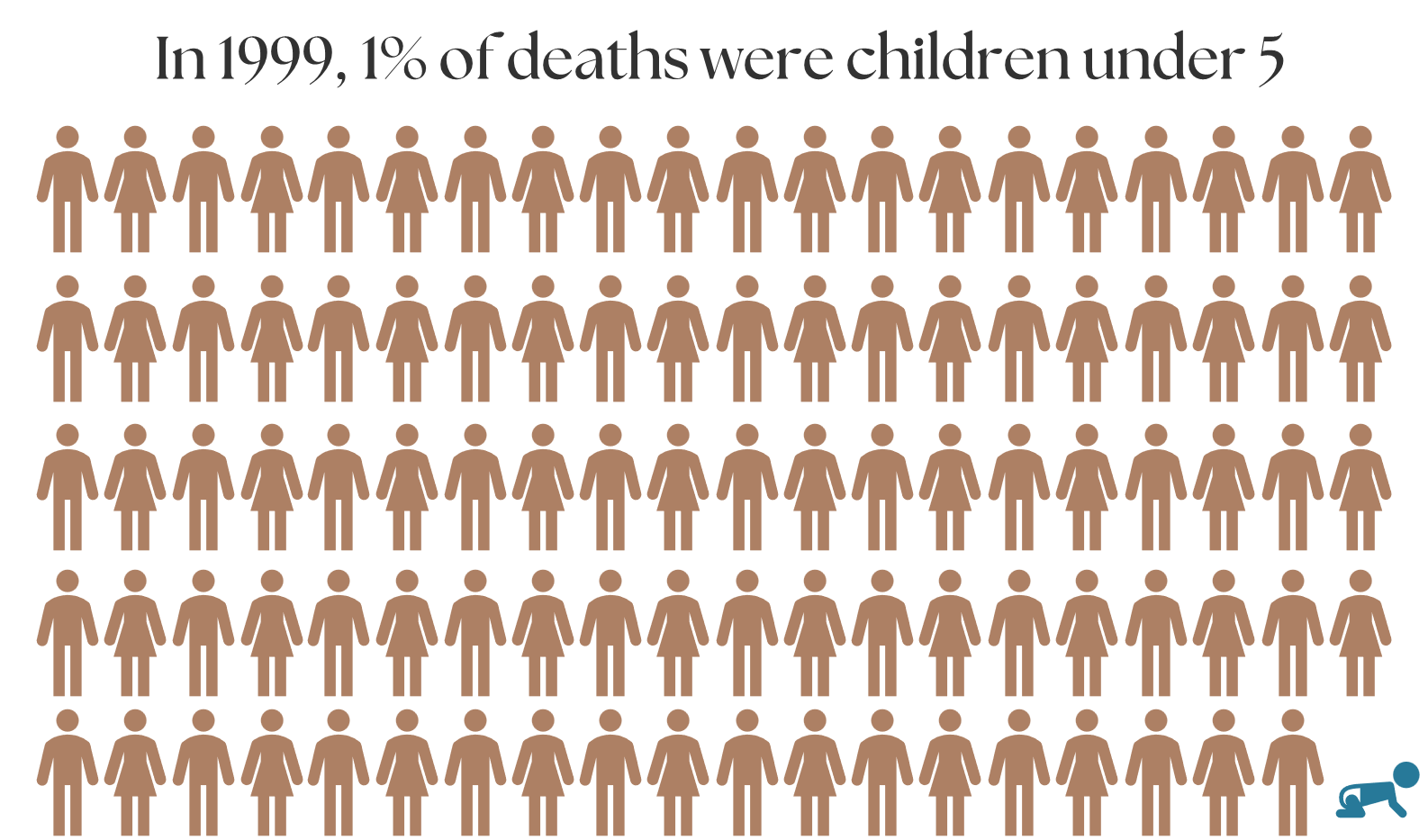
But we’ve collectively forgotten that in 1900, 30% of deaths in the US were children under 5, compared to 100 years later when that percentage had plummeted to 1.4%. As the visuals below highlight, there is a huge difference between 30% of deaths being attributed to children under 5, and only 1% of deaths being attributed to this same age range. Vaccines were a large contributor to the reduction, along with improvements in sanitation and the advent of antibiotics.

Vaccines hugely reduced deaths and hardships associated with diseases like diphtheria, polio, and measles
I was struck by an article last fall that called attention to the fact that most people don’t even know what diphtheria is anymore because it’s now a vaccine-preventable illness that is almost never contracted in the US. But it hasn’t always been that way.
In short, the death rate from diphtheria plummeted almost 100% (99.996%, to be exact) once a vaccine for this horrific disease, which effectively ate away at the throat lining and killed up to 20% of those it infected, was universal in the 1940s. The table below highlights its impact over a century.
| 1919 | 2019 | |
| Deaths from diphtheria | 14,000 | 1 |
| US child population | 35,000,000 | 73,000,000 |
| % of children dying from diphtheria each year | 0.04% | 0.0000014% |
If we didn’t have the vaccine we do today, we’d lose approximately 29,000 children to diphtheria each year in the US. (This is based on the number of children in the US today multiplied by the death rate before the diphtheria vaccine.)
Now, let’s look at a similar story with measles. While less deadly than diphtheria, contrast the chart below looking at measles cases and hospitalizations before a vaccine with those after it was widespread. In fact, the difference is so stark it’s almost impossible to see on a chart where the pre-vaccine numbers are included.
Annual measles cases and hospitalizations in the US, pre-vaccine and post-vaccine
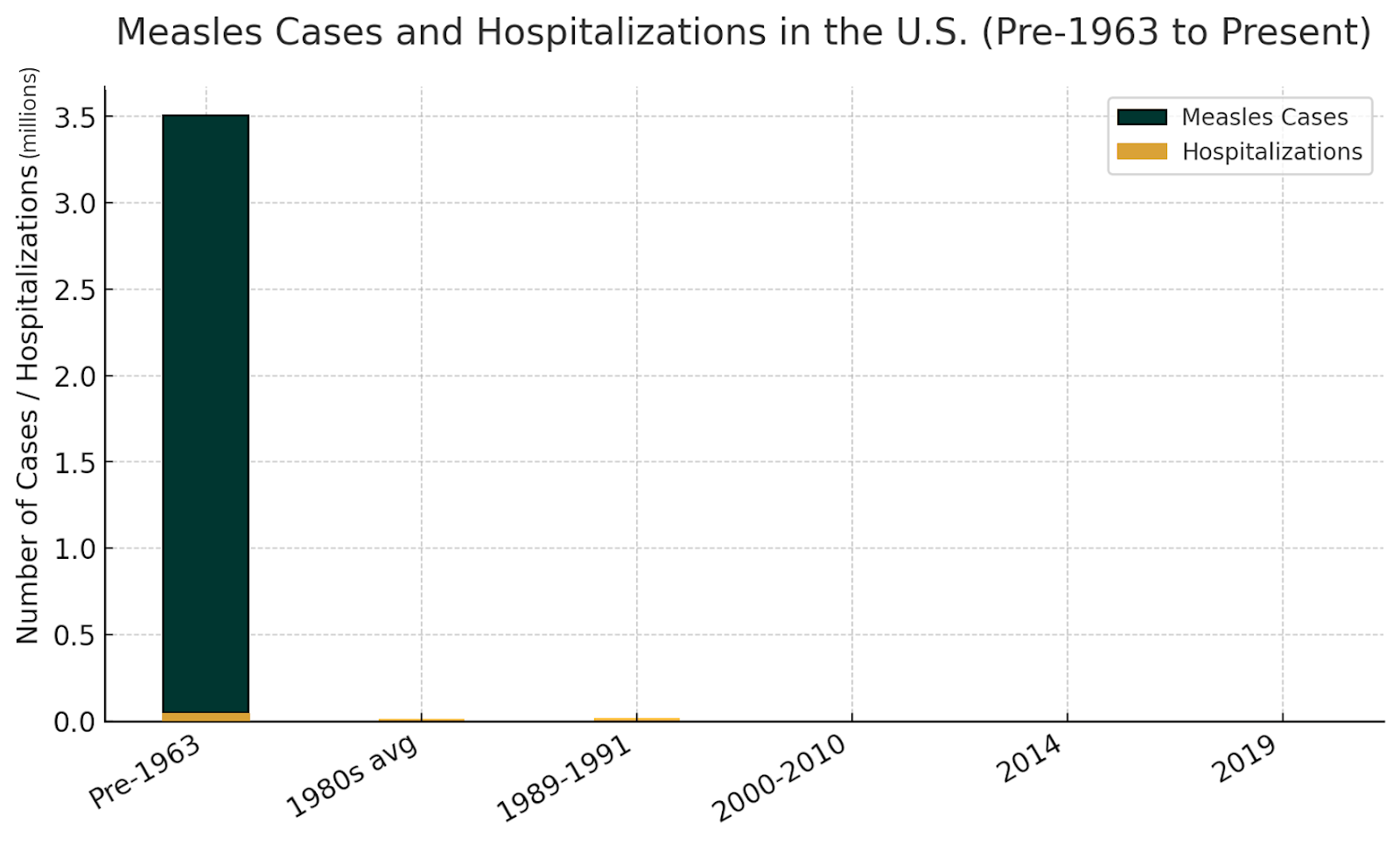
According to the CDC, before the measles vaccine, there were 3-4 million measles cases and 48,000 hospitalizations from measles each year.
Annual measles cases and hospitalizations in the US, post-vaccine
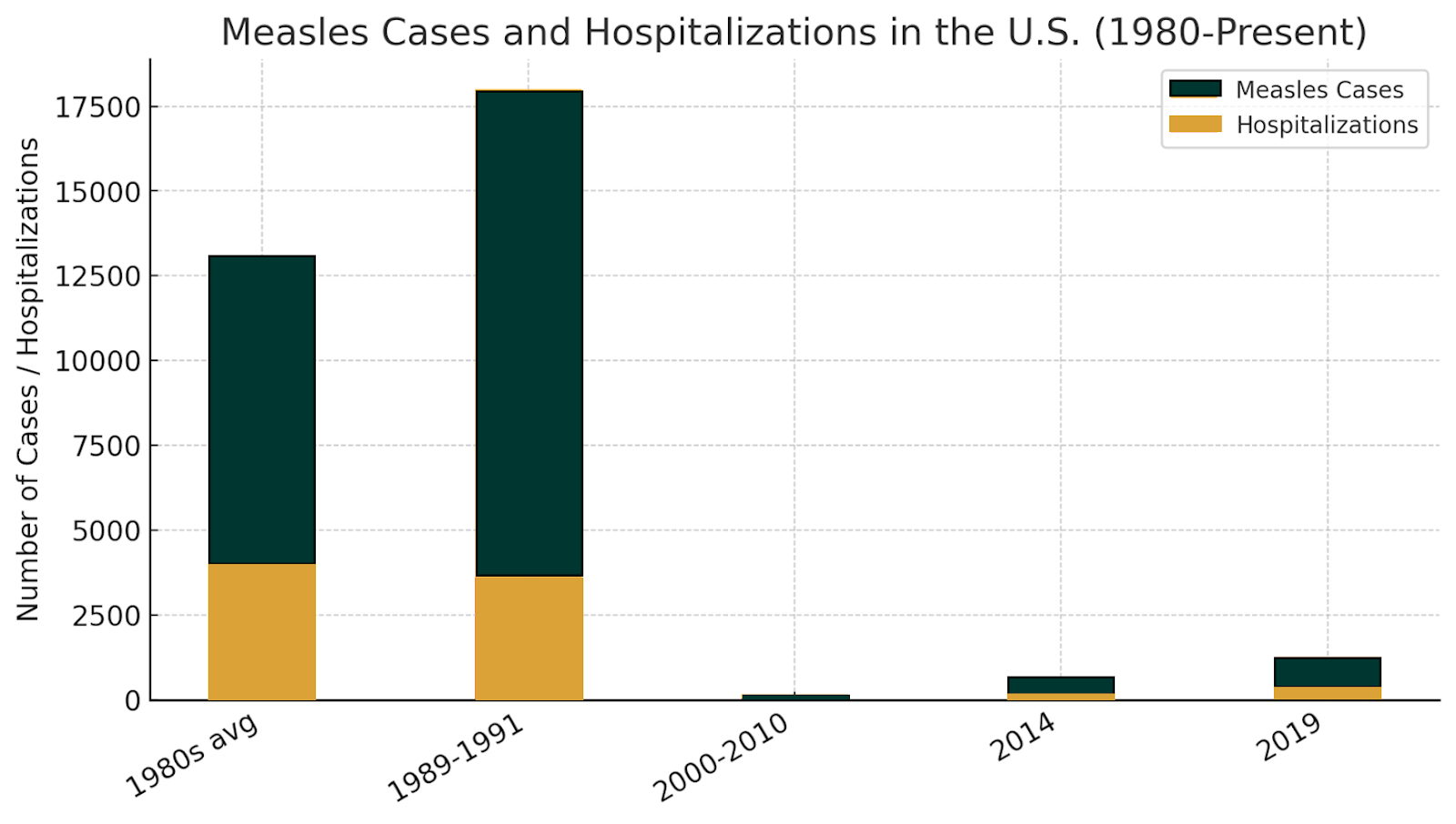
Originally, one dose of the MMR vaccine was given. But after a 1989-1991 outbreak in vaccinated children, a second vaccine dose became the norm. This change led to measles elimination in the US in 2000. The subsequent upticks in cases and hospitalizations in 2014 and 2019 were due to outbreaks in unvaccinated people in under-vaccinated communities. Notably, another outbreak is occurring now in Texas, with at least 48 cases and 13 hospitalizations so far. This is completely preventable.
As these charts and statistics highlight, childhood vaccines significantly reduced deaths, hospitalizations, and illnesses across the nation.
Lest we think vaccine skepticism is going to be short-lived or is simply a trend of the day, Jessica Grose reminded us back in October, “the trust in public health remains shaky. Whether or not Trump wins or gives Kennedy a position of power in his administration, the desire to sow doubt in our medical system will outlast them both.” As I called out before, she’s right.
So, we need a new strategy. One that acknowledges the fears people have and those they’ve forgotten, while also speaking to the progress they seek.
Where we go from here: To raise the number of vaccinated children, we have to speak to parents’ Jobs to Be Done
Our collective amnesia of a deadly past is only part of our current circumstance. While it’s a critical one to remind parents about, public health communicators must also understand more about hesitant parents’ current situations and acknowledge their desires for progress on social, emotional, and functional dimensions.
Said differently, those interested in protecting and promoting public health and overall population health must communicate differently to reach and persuade those who are uncertain if vaccines are right for their families.
There are a number of pathways for this. One, grounded in the tenets of Jobs to Be Done, is proposed here. In practice, it might look like the following:
- Understand parents’ fears: Start from a position of respect. Ask questions and truly listen to the parents’ answers. Their fears are valid, and they’re a barrier to herd immunity, even if they aren’t grounded in scientific evidence.
- Speak to the functional outcomes parents seek: Almost every parent wants what’s best for their children. Providers and public health messengers must acknowledge this as they speak to parents.
- While respecting their fears or uncertainties, state bluntly the risks of hospitalization and death when children contract vaccine-preventable diseases.
- Tap into parents’ desires to do what’s best for their child and explain that childhood vaccines are part of the critical path to ensure childhood survival.
- Understand and speak to social and emotional outcomes: The functional outcome (help my child survive) is only one driver of vaccination. There are also social factors, such as how parents will be perceived in their families or communities, or even how they’re perceived by their pediatrician, that drive parents to choose vaccination or not. Additionally, there are emotional drivers. Fear of negative side effects is one emotional driver, but talking to parents will help messengers understand and address the others as well.
Only with a clear understanding of where people are coming from and what outcomes they seek can we effectively communicate to change their behavior. This isn’t a guess or a nice idea. It’s a theory. And theories help us predict the future.
In this circumstance, it’s clear. What got us here won’t get us there. Assuming our children will survive childhood isn’t a given. So now’s the time to dig deeper and uncover the language and motivations behind why parents are firing vaccines. Continuing to say they “save lives” and are “safe and evidence-based” may be necessary, but it’s not sufficient. And sufficient is required for survival.
We don’t have time to wait. Our children’s future—and our own—is hanging in the balance.
