
Chronic diseases account for seven in ten deaths in the United States, with heart disease, obesity, cancer and type 2 diabetes numbering among the most common. That list is likely to grow as the population ages, and scientific advances continue to transform terminal conditions into ones people can live with (if often uncomfortably) for months or years. To reduce the terrible human and economic costs of chronic disease, our healthcare system must learn to facilitate positive change in individual behavior, which has the greatest impact on health status and longevity of any contributing factor—including healthcare—by a long-shot.
This is an arduous task. For despite proven, widely-known methods of ameliorating some of the most deadly, burdensome and costly chronic conditions of our time—quit smoking, drink less, eat nutritiously, exercise regularly and take prescribed medications—millions of people fail, every day, to do what they know is good for them.
Why? It isn’t that people don’t care about their health. Surveys and the $500+ billion consumer health and wellness market say people do care, a lot. Rather, people and life are complicated. So people find themselves absorbed in other problems, swept up by other ambitions, or trying to adopt healthcare regimes that don’t fit their circumstances, rather than making the positive changes nobody can make for them.
In this context, our cross-industry innovation research, coupled with numerous healthcare provider interviews, indicates that people’s conscious health decisions are surprisingly like consumer-goods purchase decisions. Specifically, both types of decisions are influenced by a constellation of factors beyond the “objective” merits of the solution under consideration. In Health for Hire: Unleashing Patient Potential to Reduce Chronic Disease Costs, Clayton Christensen, Andrew Waldeck and I explore some of the most influential factors, and how the Theory of Jobs to Be Done can help providers and patients address them to facilitate positive change in health behaviors.
One finding we share is that people’s unique beliefs about health—what it means, what it takes, whether it is desirable or attainable—are among the most influential factors affecting health decisions. We’ve synthesized what we’ve learned about health beliefs into a notion we call the Health Reference Point.
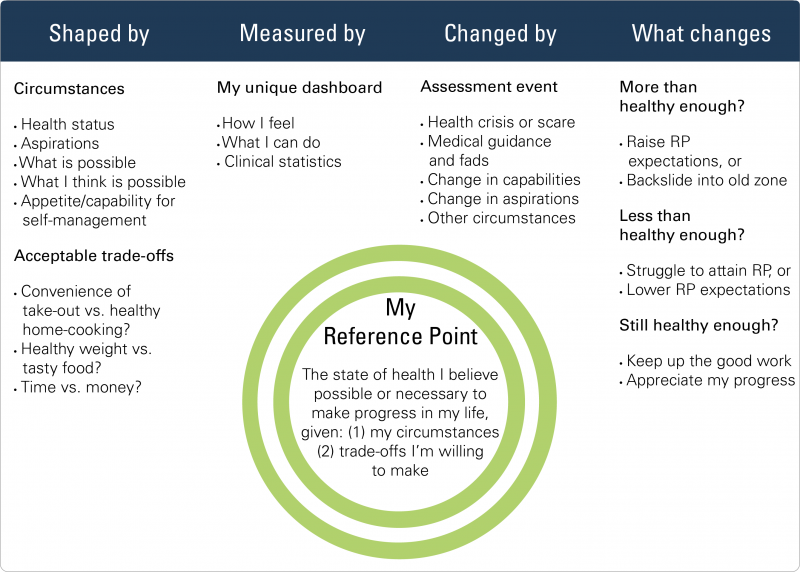
A Health Reference Point is the level of mental, emotional, and physical health people believe possible or necessary to make the progress they seek, at a particular life juncture, given their circumstances and the trade-offs they are willing to make. Everybody has a Health Reference Point, whether they know it or not. It is the inner benchmark we measure ourselves against when someone asks, “How are you doing?” or when we’re considering whether we need to “up our health game,” and whether that’s possible given the effort we’re willing and able to expend in order to do so.
The Health Reference Point is shaped by an individual’s holistic inner and outer experience, including their clinical health status. And for each individual, it translates into a set of personal, circumstance-dependent health measures. For example, in our research we learned about an elderly, wheelchair-bound amputee on oxygen. While his physical condition was limiting, he managed to remain socially active, and enjoyed volunteering regularly for local causes. “As long as he can get out in the community and do all that, he feels healthy,” his physician told us. “So, if he’s up to it and his numbers are stable, I say, ‘You’re doing great!’”
Such focus also reveals patients’ intellectual barriers to health improvement, enabling providers and patients to openly challenge them. In the context of a trusting relationship over time, doing so can open up more opportunities for health improvement, as unproductive assumptions about what’s possible and beneficial gradually fall away.
Extensive media coverage and policy discourse on drugs and medical technology might suggest that these cost drivers are the biggest lever the industry has to pull in the quest to make healthcare more affordable. But individuals too represent great, untapped potential for reducing costs— specifically, the human and economic costs of chronic disease—through more effective self-management.
Providers can help unleash this potential by collaborating with patients to create health solutions they have the capacity to embrace, not only given their unique circumstances, but also in context of their evolving beliefs about health. The Health Reference Point is a valuable tool toward that end.
For more about innovation in healthcare, see:
How Disruption Can Finally Revolutionize Healthcare