
If you’re reading this, you likely work in health care, public health, or care about one or both of these topics. You’ve likely also seen the vast array of pieces on RFK Jr.’s baseless claims about vaccines. So, what’s different about this piece? This isn’t an opinion or even a recap of what the data says because you already know that. It’s a theory-based analysis.
Since data hasn’t swayed RFK, Jr.’s approach to vaccines, I’m leveraging the power of theory to discuss the likely outcomes of his impact on public health in the years to come.
Why? There are two reasons. The first is that theory is a powerful predictor of the future. Second, you may have the ability to sway his opinion.
In this case, theory can reveal how to prevent a big public health disaster by predicting the one we appear to be voluntarily opting into.
What exactly do I mean?
On November 14th, Donald Trump announced that he selected RFK, Jr. to lead the Department of Health and Human Services. Others have noted that for a variety of reasons—including a lack of experience, expertise, and knowledge—he is a questionable, if not completely dangerous, selection. Many have also recapped why decades of medical practice and reduction in death rates suggest his perspectives pose a serious risk to population health and could revitalize diseases like diphtheria.
As highlighted in an NBC interview after Trump’s election victory, RFK, Jr.’s point of view on vaccines reflects his lack of understanding about how public health works. In brief, RFK, Jr. stated, “If vaccines are working for somebody, I’m not going to take them away…People can make individual assessments about whether that product is going to be good for them.”
RFK, Jr. proposes—or at least he currently claims—that “people ought to have choice and that choice ought to be informed by the best information.” Kennedy is well-known for being a vaccine skeptic and spreader of vaccine misinformation. However, it’s been well-documented that his claims about vaccines causing autism are baseless and untrue.
Given the gap between decades of scientific evidence, public policy, medical advice, and what Kennedy purports to be true, our collective health may be in quite a bit of trouble if his appointment is confirmed. The damage spreading misinformation can do in the short run takes a long time to correct. Lest we forget, we are still recovering from the lost trust in scientists and medical professionals that resulted from misinformation amidst the COVID-19 pandemic, as well as the decline in childhood vaccinations that occurred during that time.
While the past doesn’t always predict the future, sound theory can. It allows us to foreshadow what will happen and what will not.
Modularity Theory
Modularity Theory is a theory of innovation and performance often used by entrepreneurs and business leaders. It explains that a system’s architecture determines its components and systems and defines how they must interact—fit and work together—in order to achieve desired outcomes.
The place where any two subsystems fit together is called an interface. A system’s architecture is interdependent at the interface if one part can’t be made independently of the other. Therefore, the way one part is designed and made depends on the way the other is designed and made. Unpredictable interdependencies require the same person, team, or organization to simultaneously develop both components for the whole system to work.
In contrast, a modular interface is one in which there are no unpredictable interdependencies between subsystems, people, teams, or organizations. Modular components and subsystems fit and work together in well-understood and highly-defined ways. A modular system architecture specifies the fit and function of all elements so completely that it doesn’t matter who makes the components or subsystems as long as they meet specifications.
So, to the extent that interfaces are specifiable, verifiable, and predictable, they are modular. Systems that rely on modular interfaces allow people in separate teams or organizations to do their work with little to no effort spent on coordination.
If we apply this theory to public health, let’s view government, policy, and public leadership as system architects and human populations as systems. How individuals (i.e., the “subsystems”) interface and interact with one another is unpredictable because of each person’s individual and differentiating behavior. The result? Our interactions aren’t fully specifiable, verifiable, or predictable. Therefore, we must treat our collective population as the interdependent system that it is.
However, as any local, state, or federal leader understands, this unpredictable behavior is kept in check by law, policy, and cultural norms to ensure society, or the system, functions optimally. These mandates and understandings are the architecture that underwrites performance. Remove these mandates and understandings, and the system ceases to function efficiently toward progress or success. When it comes to our health, “success” or “progress” could be defined as living long and healthy lives.
How Modularity Theory applies to vaccination
Unfortunately, due to the interdependence among individuals, theory confirms that vaccines aren’t a place where “do what works for you” is a good approach for a system population. It’s a fact that people are at risk of contracting any number of illnesses in their lifetime. However, removing the cultural understanding and/or the policy architecture of required childhood vaccines no longer ensures that individuals keep performing optimally (i.e., remain as healthy as possible). Therefore, removal could cripple the entire system.
Given all the dialogue around the importance of making our society more family-friendly or child-friendly, it’s counterintuitive that societal policies around childhood vaccinations, which, if reversed, would result in more childhood illness and death, are in question.
Take polio, for example, where population-wide vaccinations resulted in the wild poliovirus last being contracted in the US in 1979. This outcome wouldn’t have been possible if people only opted for the vaccine because it “worked for them.”
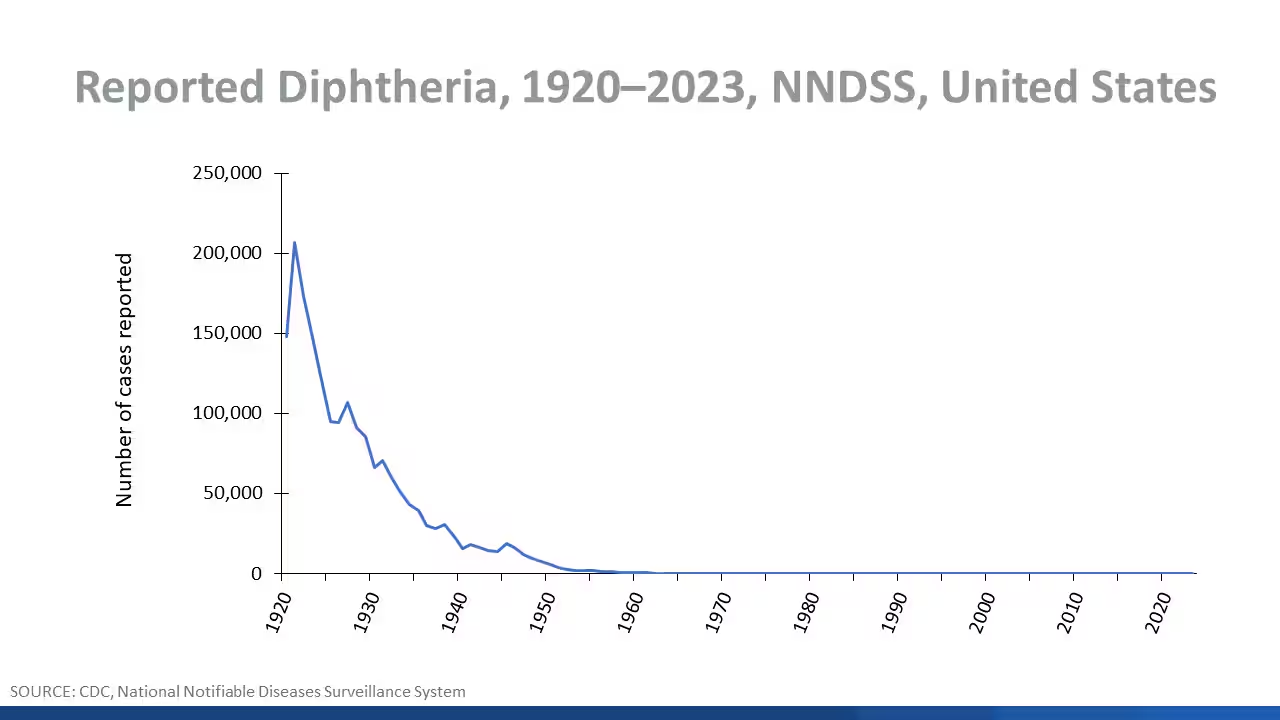
Additionally, diphtheria cases plummeted after the 1940s, when the original vaccine was created and widely adopted. The massive reduction in cases is highlighted in the CDC’s graph below. When cases fell, so did associated deaths.
Similarly, measles was eliminated from the US in 2000 due to widespread adoption of the MMR vaccine (>95%). However, when children fell behind on vaccination schedules during the COVID-19 pandemic, two-dose MMR coverage in the US fell to 92.7%, with some places below 80%. Given what we know about herd immunity and human interdependence, the result was predictable: a surge in measles cases worldwide, where vaccination rates are far below the required 95% for herd immunity.
Learning from the past to predict the future
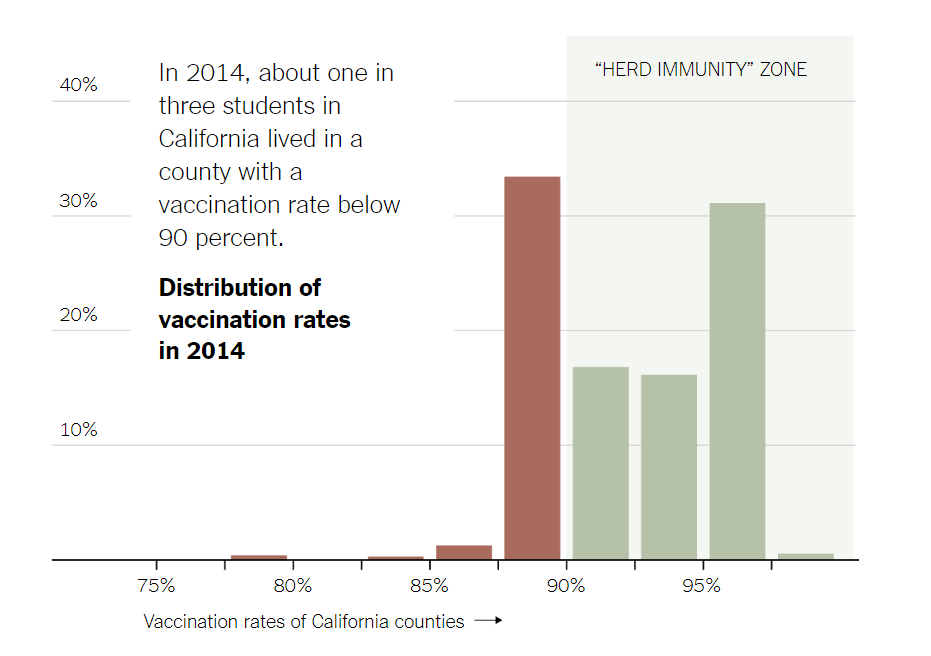
We saw a similar situation back in December 2014 in California, when 159 people contracted measles from an outbreak traced back to Disneyland. Why was there an outbreak? The chart below, from The New York Times, highlights that measles was able to infect so many people in this situation because one in three children lived in a county with a vaccination rate below 90%.
To address this issue, California instituted a policy change, which significantly increased vaccination rates in schools with the lowest rates between 2014-2016. This is a powerful story for us to remember for three reasons:
- Many vaccine-preventable illnesses rely on widespread vaccine adoption and resulting herd immunity for maximum effectiveness,
- Policy is a powerful lever for public health improvement and
- Fewer people are sick from vaccine-preventable illnesses, and fewer children die when more children get vaccinated.
These are powerful lessons to keep in mind for an incoming administration with a focus on family- and child-friendly policies. Under leadership that questions decades of proof of the efficacy, effectiveness, and benefits of widespread vaccination, decades of progress—that is, the lives saved and healthy lives created—are at risk.
But it doesn’t have to be.
Medical misinformation kills. And while childhood vaccination policies are governed at the state level, spreading misinformation from a position of power is dangerous to a system’s ability to function and, therefore, to be successful.
Where to go from here
As the head of the WHO recently noted, “Measles vaccine has saved more lives than any other vaccine in the past 50 years…To save even more lives and stop this deadly virus from harming the most vulnerable, we must invest in immunization for every person, no matter where they live.”
We are interdependent beings. More people getting vaccinated is better for our collective health and, therefore, our performance as a society than fewer people getting vaccinated. Public officials who disagree with this pose a risk to our individual, collective, and future well-being.
Therefore, I hope we realize how our policies and choices impact the entirety of our interdependent system.
We don’t exist in a vacuum. Our decisions impact other people’s lives and livelihoods. We’d be wise to have our public policies support this truth and, therefore, to individually act accordingly.
Because theory foreshadows exactly what will happen if we don’t…
